
Pharmacology is the science dealing with drugs.
Two branches:
- PharmacoKinetics → Effect of Body on Drug
- PharmacoDynamics → Effect of Drug on Body
Drug:
Drug is a substance which is intended to be used to modify or explore the physiological function or pathological state
for the benefits of recipient.
Risk benefit ratio:
If it is favorable, then drug is used e.g. Streptokinase is used in MI but not for peripheral vascular disease
Essential drugs
These are the drugs that cater to priority health care needs of a population.
These drugs should be
– Always available
– – In adequate quantity
– – With assured quality
Mostly available as single compound.
Orphan drugs-
– These are drugs for which the expenditure done for the development of the drug is unlikely to be recovered from sale of the drug.
– Include drugs which are used for rare diseases.
– Also include drugs for relatively common diseases in third world; countries with less paying capacity.
Route Angle of needle with horizontal Advantage
Intravenous 25 degree Used in Emergencies
Intramuscular 90 degree —-
Subcutaneous 45 degree Self-administration possible
Intradermal Almost 0 degree For BCG and Allergy testing
Intravenous route can be of two types:
- Bolus
- Infusion
– Because the drug is directly entering the systemic circulation, any volume of fluid can be given by intravenous route.
– Titration is possible by intravenous route
– Disadvantages of intravenous route are:
- Sterile precautions should be followed
- Require an expert person for administration
- It is costly
– By Intramuscular route, maximum 5-10 ml volume can be given.
Pharmacokinetics: Absorption
Pharmacokinetics
Pharmacokinetics refers to the movement of a drug within the body and includes four key processes:
1. Absorption – The process by which a drug enters the bloodstream. IV administration bypasses absorption since the drug is directly introduced into circulation.
2. Distribution – The transport of the drug from the bloodstream to tissues and organs. Factors like blood flow, protein binding, and tissue permeability influence distribution.
3. Metabolism – The biotransformation of the drug, primarily in the liver, where enzymes convert it into active or inactive metabolites.
4. Excretion – The elimination of the drug and its metabolites, mainly through the kidneys (urine) or liver (bile/feces), but also via sweat, saliva, or lungs (exhalation).
Absorption
Absorption is the process by which a drug moves from its site of administration into the bloodstream. It is influenced by several factors, including the drug’s formulation, route of administration, and physiological conditions.
Factors Affecting Absorption:
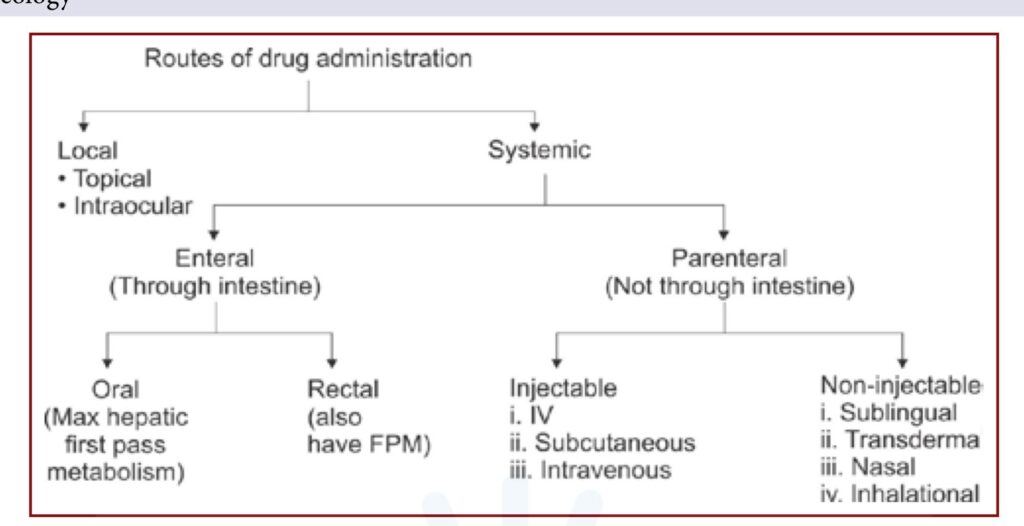
1. Route of Administration:
• Intravenous (IV): No absorption phase; the drug directly enters circulation.
• Oral (PO): Absorption occurs in the gastrointestinal (GI) tract, affected by gastric pH, food, and first-pass metabolism.
• Intramuscular (IM) & Subcutaneous (SC): Absorption depends on blood flow to the injection site.
2. Drug Properties:
• Lipid-soluble drugs absorb faster than water-soluble ones.
• Small, non-ionized molecules cross membranes more easily.
3. Blood Flow to the Absorption Site:
• Increased blood flow (e.g., in muscles) enhances absorption.
• Decreased blood flow (e.g., in shock or low-perfusion states) slows absorption.
4. Surface Area for Absorption:
• The small intestine has a large surface area, making it the primary site for oral drug absorption.
5. First-Pass Metabolism (for Oral Drugs):
• Some drugs are metabolized in the liver before reaching systemic circulation, reducing their bioavailability.
Henderson Hasselbach Equation
The Henderson-Hasselbalch equation is used to determine the pH of a solution based on the concentration of an acid and its conjugate base. It is commonly used in pharmacology to understand drug ionization and absorption.
Equation:
Where:
• pH = the acidity of the solution
• pKa = the acid dissociation constant (the pH at which 50% of the drug is ionized)
• [A⁻] = concentration of the conjugate base (ionized form)
• [HA] = concentration of the weak acid (unionized form)
Pharmacological Application:
• Drug Absorption: Weak acids (e.g., aspirin) are better absorbed in acidic environments (stomach) because they remain unionized. Weak bases (e.g., morphine) are better absorbed in alkaline environments (intestine).
• Ion Trapping: Drugs can become trapped in certain compartments based on pH differences, affecting their distribution and elimination.
Acidic Drug [Aspirin], mainly absorbed from stomach
Basic Drug [Morphine] mainly absorbed from intestine
But practically all drugs (even acidic drugs like aspirin) are absorbed more from intestine as compared to stomach
because:
- Large surface area of intestine
- Longer time drug stays in intestine
Bioavailability
Bioavailability
Definition:
Bioavailability refers to the fraction (F) of an administered drug that reaches the systemic circulation in its active form. It is expressed as a percentage (%) and is a key factor in drug dosing.
Factors Affecting Bioavailability:
1. Route of Administration:
• Intravenous (IV): 100% bioavailability (F = 1) since the drug directly enters circulation.
• Oral (PO): Typically lower due to first-pass metabolism and incomplete absorption.
• Other Routes (IM, SC, inhalation, etc.): Varies depending on absorption efficiency.
2. First-Pass Metabolism:
• Drugs taken orally pass through the liver before reaching circulation, which can metabolize and reduce the amount of active drug available.
• Example: Propranolol has low oral bioavailability due to extensive first-pass metabolism.
3. Drug Solubility & Formulation:
• Lipid-soluble drugs cross membranes easily, increasing bioavailability.
• Drug formulation (e.g., extended-release, enteric coating) can alter absorption.
4. Gastrointestinal Factors:
• pH, food interactions, enzyme activity, and gut microbiota can affect drug absorption.
Bioavailability Calculation:
For oral drugs, bioavailability is calculated as:
Where AUC (Area Under the Curve) represents drug exposure over time.
It is the fraction of given dose which that reaches the systemic circulation
in unchanged form
→ Bioavailability → Determines the Dose
High bioavailability → Low Dose
Low bioavailability → High dose
Factors affecting:
- Absorption
↑ Absorption → ↑ Bioavailability
↓ Absorption → ↓ Bioavailability
- Route of Administration
Route % Bio-availability Fractional Bio-availability
Oral 5-100 0.05 < F < 1
I.M. 75-100 0.75 < F < 1
S.C. 75-100 0.75 < F < 1
IV 100 1 - First Pass metabolism/Pre systemic metabolism
↑ First Pass metabolism → ↓ Bioavailability
↓ First Pass metabolism → ↑ Bioavailability
NTG [Nitroglycerine]
Nitroglycerin (NTG)
Class: Nitrate (Vasodilator)
Uses:
• Angina (chest pain)
• Heart failure
• Hypertensive emergencies
Pharmacokinetics:
• Absorption: Highly lipophilic, rapidly absorbed through mucosal membranes.
• Bioavailability: Extremely low (~10-20%) when taken orally due to extensive first-pass metabolism in the liver.
• Metabolism: Metabolized in the liver by nitrate reductase into inactive metabolites.
• Excretion: Primarily via urine.
Routes of Administration:
1. Sublingual (SL) Tablets or Spray:
• Avoids first-pass metabolism, providing rapid onset (1-3 min)
• Used for acute angina relief
2. Transdermal Patches/Ointment:
• Provides sustained release for chronic angina prevention
3. Intravenous (IV):
• Used in acute coronary syndromes or hypertensive emergencies
4. Oral Tablets (Extended Release):
• Less commonly used due to low bioavailability
Key Considerations:
• Tolerance: Continuous use can lead to nitrate tolerance. A nitrate-free interval (e.g., 8-12 hours at night) is recommended.
• Side Effects: Headache, hypotension, dizziness, reflex tachycardia.
• Contraindications:
• Phosphodiesterase-5 inhibitors (e.g., sildenafil, tadalafil) – can cause severe hypotension.
• Severe hypotension or hypovolemia.
Bioequivalence (Biologically Equivalent)
Bioequivalence (Biologically Equivalent)
Definition:
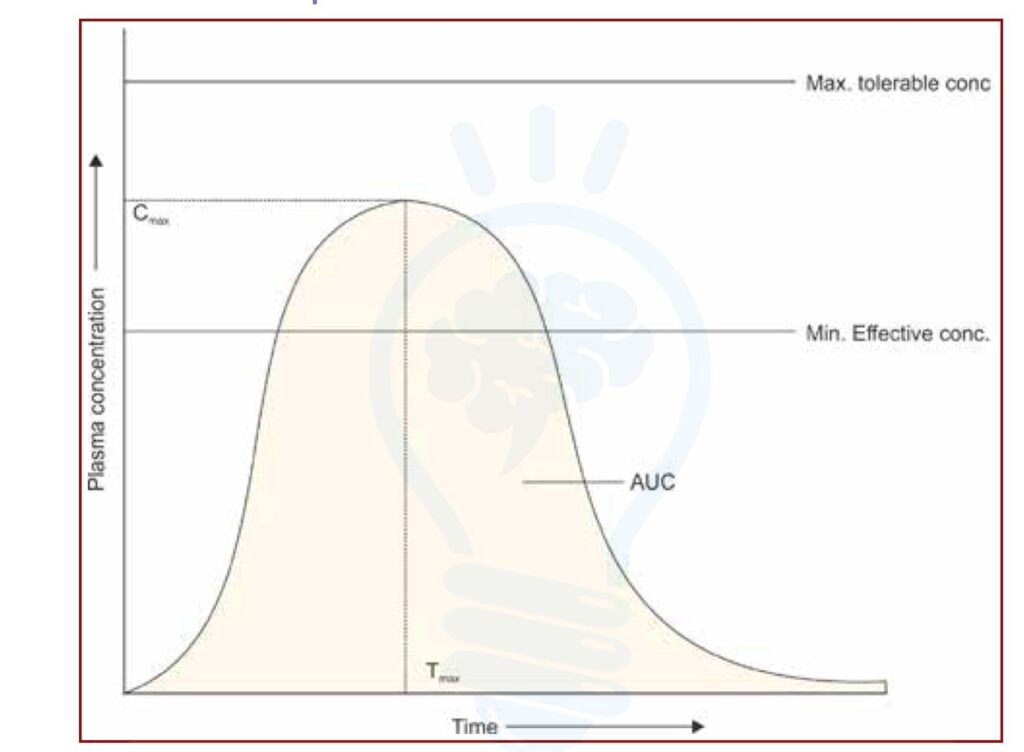
Two drug formulations are considered bioequivalent if they have comparable bioavailability and produce the same therapeutic effect at the same dose. This means they have similar rate (Cmax, Tmax) and extent (AUC) of absorption when administered under the same conditions.
Key Parameters for Bioequivalence:
1. Peak Plasma Concentration (Cmax): Maximum drug concentration in the blood.
2. Time to Peak Concentration (Tmax): Time required to reach Cmax.
3. Area Under the Curve (AUC): Total drug exposure over time.
Regulatory Criteria:
• Bioequivalence is established if the 90% confidence interval (CI) for Cmax and AUC falls within 80-125% of the reference drug (as per FDA and EMA guidelines).
• This ensures generic drugs provide the same therapeutic effect as brand-name drugs.
Example:
• Brand: Plavix (Clopidogrel) vs. Generic Clopidogrel
• If the generic drug has a Cmax and AUC within 80-125% of Plavix, it is considered bioequivalent and interchangeable.
– 2 brands of same drug are compared
- If two brands of same drug have almost similar bioavailability (20%), these are called bioequivalent
- Most of the drugs are bioequivalent except phenytoin
Plasma Concentration Vs Time Graph
Pharmacokinetics: Distribution
Pharmacokinetics: Distribution
Definition:
Distribution refers to the process by which a drug is transported from the bloodstream to various tissues and organs in the body. It determines how much of the drug reaches its site of action.
Factors Affecting Drug Distribution:
1. Blood Flow:
• Highly perfused organs (brain, liver, kidneys) receive the drug faster.
• Poorly perfused tissues (fat, muscle, bone) receive the drug more slowly.
2. Plasma Protein Binding:
• Drugs bind to proteins like albumin (for acidic drugs) or α1-acid glycoprotein (for basic drugs).
• Only free (unbound) drug is pharmacologically active.
• High protein binding can prolong drug action and reduce clearance.
3. Tissue Binding & Storage:
• Some drugs accumulate in tissues (e.g., fat, bone), leading to delayed elimination and prolonged effects.
• Example: Tetracyclines bind to calcium in bones and teeth.
4. Volume of Distribution (Vd):
• A theoretical parameter that indicates how widely a drug distributes in the body.
• High Vd (>40 L): Drug extensively distributes into tissues (e.g., lipophilic drugs like amiodarone).
• Low Vd (<10 L): Drug remains mostly in plasma (e.g., heparin).
5. Blood-Brain Barrier (BBB) & Placental Barrier:
• Only lipophilic, small, and non-ionized drugs can cross the BBB (e.g., benzodiazepines).
• The placenta allows some drugs to cross, affecting fetal exposure.
Example Drugs & Their Distribution:
• Warfarin: Highly protein-bound, stays in plasma (low Vd).
• Aminoglycosides: Distribute mainly in extracellular fluid (moderate Vd).
• Lipid-soluble drugs (e.g., Propofol): Rapidly distribute into tissues, causing a short duration of action.
Factors affecting:
- Lipid Solubility
→ Most important Factor
Lipid soluble Drugs → Higher Distribution
Water Soluble Drugs → Lower Distribution - Plasma Protein Binding (PPB)
↑ PPB → Low Distribution
→ Acidic drugs bind to → Albumin
→ Basic drugs bind to → a1 Acid Glycoprotein
→ Different drugs have different percentage of binding
Acidic drugs
Aspirin
Barbiturates
Methotrexate
Bind to : Albumin
Mnemonic : Salt with cations like Na+ & K+ e.g., Phenytoin sodium
Basic drugs
Atropine
Morphine
Amphetamine
Bind to : α-1 acid Glycoprotein
Mnemonic : Drugs ending with ‘INE’
Salts with anions like Ipratropium bromide
Importance of PPB
a. Distribution:
→ if PPB is high, its volume of distribution (Vd) → ↓↓
b. Duration:
→ If drug has ↑ PPB Duration of action of drug ↑, because plasma protein to which it is bound serves as storage site.
c. Displacement interactions:
→ PPB sites on albumin & α1 – Acid glycoprotein arenon -specific
→ One drug may displace another drug leading to increase in free concentration of latter. This may result in toxicity.
→ For example, Warfarin is displaced by sulfonamides leading to bleeding.
d. Dialysis:
→ If a drug has ↑ PPB; dialysis of that drug cannot be done
→ Because proteins are not filtered during dialysis; thus the drug with ↑ PPB is retained along with plasma proteins
e. Filtration:
→ If, drug has ↑ PPB, its filtration would be lesser.
- Barriers
– Brain is bound by Blood Brain Barrier.
– In circumventricular Organs, this barrier is absent.
– CTZ [chemoreceptor Trigger Zone] is important circumventricular organ.
– Vomiting not caused by → Anti-emetics and Anti-psychotics
Volume of Distribution (Vd)
→ Volume of Distribution Vd ∝ Amount of Drug in Tissues
More Vd → More distribution
Chloroquine
Drug with maximum Vd [> 1300 L]
Mostly distributed in Liver but site of preferred action is RBC
Loading Dose [LD]
Initial high dose given to start the action
LD = Vd x Target Plasma Concentration
Maintenance Dose
Repeated doses given to maintain the plasma concentration.
MD = CL x Target PC
Pharmacokinetics: Metabolism
Pharmacokinetics: Metabolism
Metabolism is one of the key processes in pharmacokinetics, referring to the biochemical transformation of drugs within the body. It primarily occurs in the liver, though other tissues like the intestines, kidneys, lungs, and plasma also contribute. The goal of metabolism is usually to convert lipophilic drugs into more hydrophilic compounds for easier excretion.
Phases of Metabolism
Metabolism occurs in two main phases:
Phase I (Functionalization Reactions)
• Purpose: Introduces or uncovers functional groups (-OH, -NH2, -SH, -COOH) to increase polarity.
• Enzymes: Primarily catalyzed by the cytochrome P450 (CYP) enzyme family, along with other enzymes like flavin-containing monooxygenases (FMO) and alcohol dehydrogenases.
• Types of Reactions:
• Oxidation (e.g., CYP450-mediated hydroxylation)
• Reduction (e.g., nitroreduction)
• Hydrolysis (e.g., ester or amide hydrolysis by esterases)
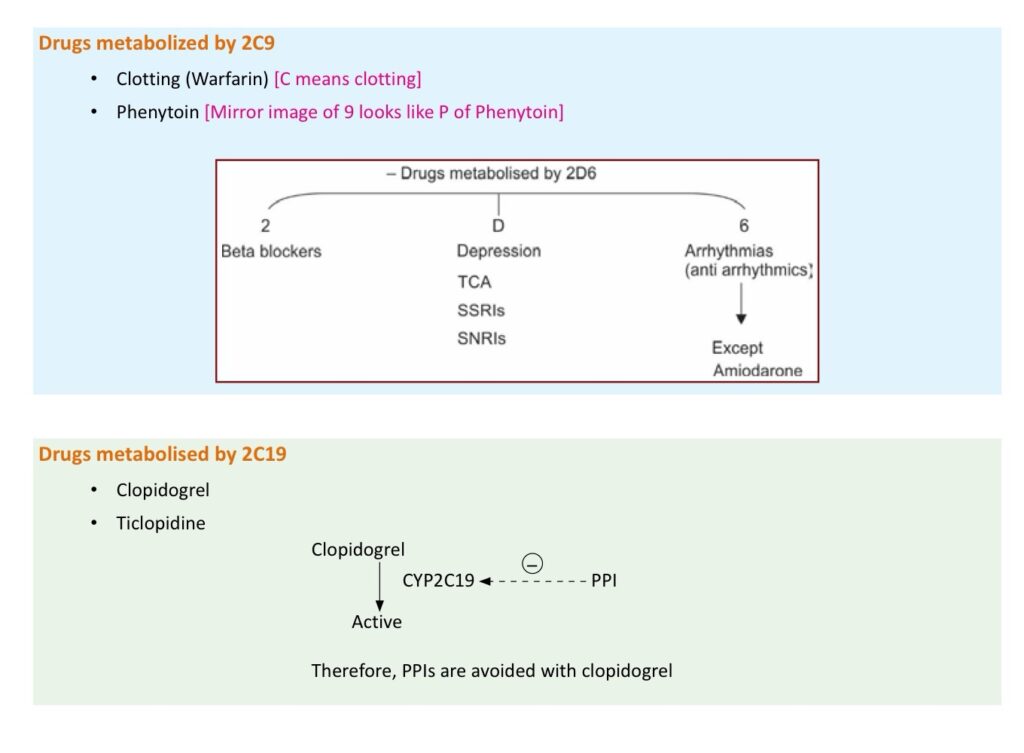
• Example: Conversion of codeine to morphine by CYP2D6.
Phase II (Conjugation Reactions)
• Purpose: Further increases water solubility by adding large, hydrophilic molecules.
• Enzymes: Transferases (e.g., UDP-glucuronosyltransferase [UGT], sulfotransferase [SULT], glutathione S-transferase [GST]).
• Types of Conjugation Reactions:
• Glucuronidation (e.g., bilirubin metabolism)
• Sulfation (e.g., acetaminophen metabolism)
• Glutathione conjugation (detoxification)
• Acetylation & Methylation (affects drug activity/toxicity)
• Example: Morphine glucuronidation to morphine-6-glucuronide.
Factors Affecting Drug Metabolism
1. Genetics – Variability in CYP450 enzymes (e.g., CYP2D6 poor vs. ultra-rapid metabolizers).
2. Age – Neonates have immature enzyme systems; elderly patients have reduced metabolism.
3. Liver Function – Hepatic diseases (cirrhosis, hepatitis) impair metabolism.
4. Enzyme Induction/Inhibition
• Inducers: Increase metabolism (e.g., rifampin, phenobarbital).
• Inhibitors: Decrease metabolism (e.g., grapefruit juice, ketoconazole).
5. Drug-Drug Interactions – Competing for the same enzyme can alter drug levels.
6. Diet & Lifestyle – Charcoal-broiled foods, smoking, and alcohol affect CYP activity.
Clinical Importance of Metabolism
• Prodrugs – Some drugs require metabolism for activation (e.g., enalapril to enalaprilat).
• Toxic Metabolites – Some metabolites cause toxicity (e.g., acetaminophen to NAPQI in overdose).
• First-Pass Effect – Extensive liver metabolism can reduce oral drug bioavailability (e.g., propranolol).
Pharmacokinetics: Excretion
Pharmacokinetics: Excretion
Excretion is the final step in pharmacokinetics, where drugs and their metabolites are eliminated from the body. The primary organ responsible for excretion is the kidney (renal excretion), but other routes include the biliary system (fecal excretion), lungs, sweat, saliva, and breast milk.
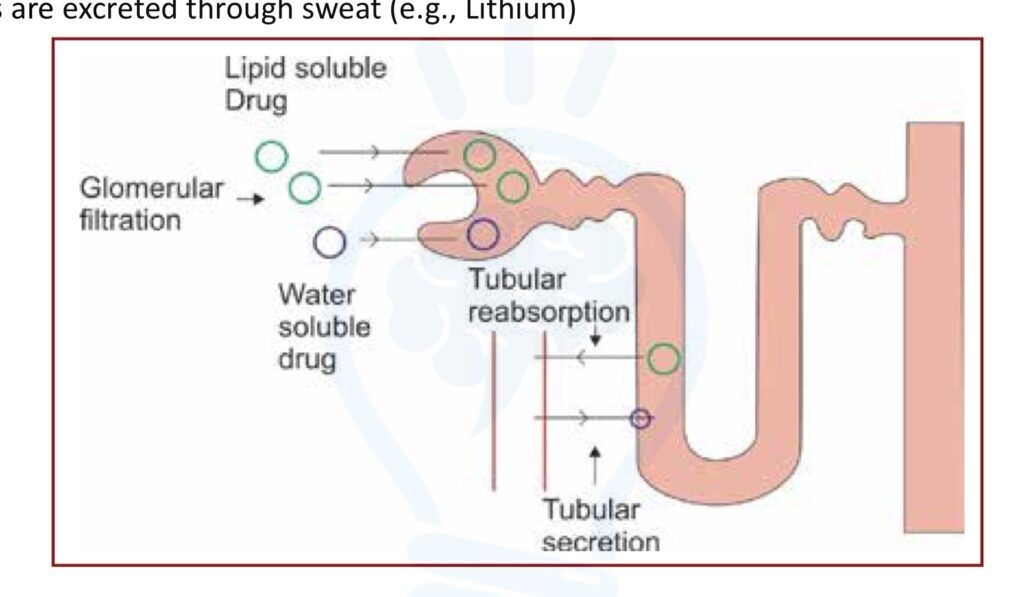
1. Renal Excretion (Most Common Route)
The kidneys eliminate drugs through three major processes:
a) Glomerular Filtration
• Mechanism: Passive filtration of free (unbound) drugs and metabolites into the renal tubules.
• Factors Affecting Filtration:
• Molecular size (small molecules pass easily).
• Protein binding (only free drug is filtered; highly protein-bound drugs are excreted more slowly).
• Glomerular filtration rate (GFR) (e.g., reduced in renal disease).
b) Tubular Secretion
• Mechanism: Active transport of drugs from blood into the renal tubules (proximal tubule).
• Key Transporters:
• Organic anion transporters (OATs) – Transport acidic drugs (e.g., penicillins, NSAIDs).
• Organic cation transporters (OCTs) – Transport basic drugs (e.g., cimetidine, metformin).
• Clinical Relevance: Drug competition at transporters can lead to drug interactions (e.g., probenecid inhibits penicillin secretion, prolonging its half-life).
c) Tubular Reabsorption
• Mechanism: Lipophilic drugs are passively reabsorbed from the tubules back into circulation.
• Factors Affecting Reabsorption:
• Urinary pH:
• Acidic urine enhances excretion of basic drugs.
• Alkaline urine enhances excretion of acidic drugs.
• Drug Lipophilicity: Non-polar drugs are reabsorbed more readily.
• Clinical Application:
• Forced diuresis & urine alkalization: Used in drug overdose management (e.g., sodium bicarbonate alkalinizes urine to enhance aspirin excretion).
2. Biliary and Fecal Excretion
• Some drugs are secreted into bile (via active transport) and excreted in feces.
• Drugs with enterohepatic circulation (e.g., estrogens, morphine) are reabsorbed, prolonging their action.
• Clinical Example: Certain drugs (e.g., rifampin) increase bile excretion, reducing the effectiveness of oral contraceptives.
3. Other Excretion Routes
• Lungs – Volatile anesthetics (e.g., isoflurane) are excreted via respiration.
• Sweat & Saliva – Minor routes; drugs like heavy metals can be detected in sweat.
• Breast Milk – Some drugs (e.g., tetracyclines, opioids) can transfer to infants.
Factors Affecting Drug Excretion
1. Renal Function – Kidney disease reduces drug clearance, requiring dose adjustments (e.g., aminoglycosides).
2. Hepatic Function – Liver impairment affects biliary excretion and metabolism.
3. Age – Neonates have immature renal function, and elderly patients have reduced clearance.
4. Urine pH & Flow Rate – Affects passive reabsorption (e.g., alkalization of urine enhances excretion of weak acids).
5. Protein Binding – Only free (unbound) drugs are excreted.
Clinical Significance of Drug Excretion
• Renal Clearance (Cl): Used to estimate how efficiently a drug is removed by the kidneys.
• Creatinine Clearance (CrCl) & Estimated Glomerular Filtration Rate (eGFR): Used to adjust drug doses in renal impairment.
• Dialysis Considerations: Drugs with low molecular weight and low protein binding are more easily removed via dialysis.
Kinetics of Elimination
Kinetics of Elimination
The elimination kinetics of a drug describes how it is removed from the body over time. This process can follow different kinetic patterns, primarily first-order and zero-order kinetics, with some drugs exhibiting mixed (Michaelis-Menten) kinetics at different concentrations.
1. First-Order Kinetics (Exponential Elimination)
• Most common type of drug elimination.
• A constant fraction of the drug is eliminated per unit time.
• Rate of elimination is proportional to drug concentration (higher drug levels = faster elimination).
• Graph (linear scale): Exponential decay curve.
• Graph (log scale): Straight line.
Key Characteristics:
• Half-life (t₁/₂) is constant, meaning the time required to eliminate 50% of the drug remains the same regardless of concentration.
• Example drugs: Most drugs, including aminoglycosides, beta-lactams, and most anesthetics.
Clinical Relevance:
• Dosing strategies: First-order drugs do not accumulate unpredictably; steady-state concentrations can be reached with regular dosing.
• Half-life calculations: Used to determine dosing intervals and time to steady state.
2. Zero-Order Kinetics (Saturation Kinetics)
• A constant amount of drug is eliminated per unit time, regardless of concentration.
• Rate of elimination is independent of drug concentration (fixed rate).
• Graph (linear scale): Straight line.
• Graph (log scale): Curved, showing non-exponential decline.
Key Characteristics:
• No fixed half-life—elimination time varies with dose.
• Occurs when elimination mechanisms (e.g., enzymes, transporters) become saturated at high drug concentrations.
• Example drugs (high doses):
• Phenytoin (anticonvulsant)
• Ethanol (alcohol)
• Aspirin (high doses)
Clinical Relevance:
• Toxicity risk: Since elimination is constant and does not scale with dose, small increases in dose can lead to drug accumulation and toxicity.
• Dosing precautions: Careful titration is required to avoid overdose.
3. Mixed (Michaelis-Menten) Kinetics
• Elimination starts as first-order at low doses but shifts to zero-order at higher doses.
• Occurs when enzymes or transporters become saturated.
• Example drugs: Phenytoin, Theophylline, Warfarin.
Clinical Relevance:
• Unpredictable elimination: Small dose increases can lead to disproportionate rises in plasma levels, requiring close monitoring.
Elimination Half-Life (t₁/₂)
• The time required for the drug concentration to decrease by 50%.
• Formula (for first-order kinetics):
Where:
• = Volume of distribution
• = Clearance
Practical Applications:
• Steady-state concentration: Achieved after ~4-5 half-lives of continuous dosing.
• Drug washout: 94% of a drug is eliminated after 4 half-lives.
Drug Clearance (Cl) and Elimination Rate
• Clearance (Cl): Volume of plasma cleared of drug per unit time.
• Total Body Clearance (Cl) = Sum of clearance from all elimination pathways (renal, hepatic, pulmonary, etc.).
Clinical Relevance:
• Used to determine maintenance doses to keep drug levels in the therapeutic range.
Summary of Key Differences
Feature
First-Order Kinetics
Zero-Order Kinetics
Elimination Rate
Proportional to concentration
Constant amount per time
Half-Life
Constant
Variable
Graph (Linear Scale)
Exponential decay
Straight line
Graph (Log Scale)
Straight line
Curved
Examples
Most drugs (e.g., ibuprofen, amoxicillin)
Phenytoin, Ethanol, High-dose Aspirin
Clinical Risk
Predictable elimination
Risk of accumulation & toxicity
Leave a Reply